
Certificate of Need Laws: The Architecture of a Healthcare Monopoly
In 35 jurisdictions, it is illegal to open a hospital, surgery center, or imaging facility without government permission. Your competitors sit on the board that decides. This is how the monopoly was built.
How Certificate of Need Works
A Certificate of Need is a government-mandated permission slip that a healthcare provider must obtain before opening a new facility, expanding services, or making significant capital expenditures. The process is designed so that your competitors decide whether you are allowed to exist.
You want to build a surgery center
You apply to the state board
Your competitors sit on that board
Your competitors vote on whether you exist

It's like asking McDonald's for permission to open a Burger King.
How We Got Here
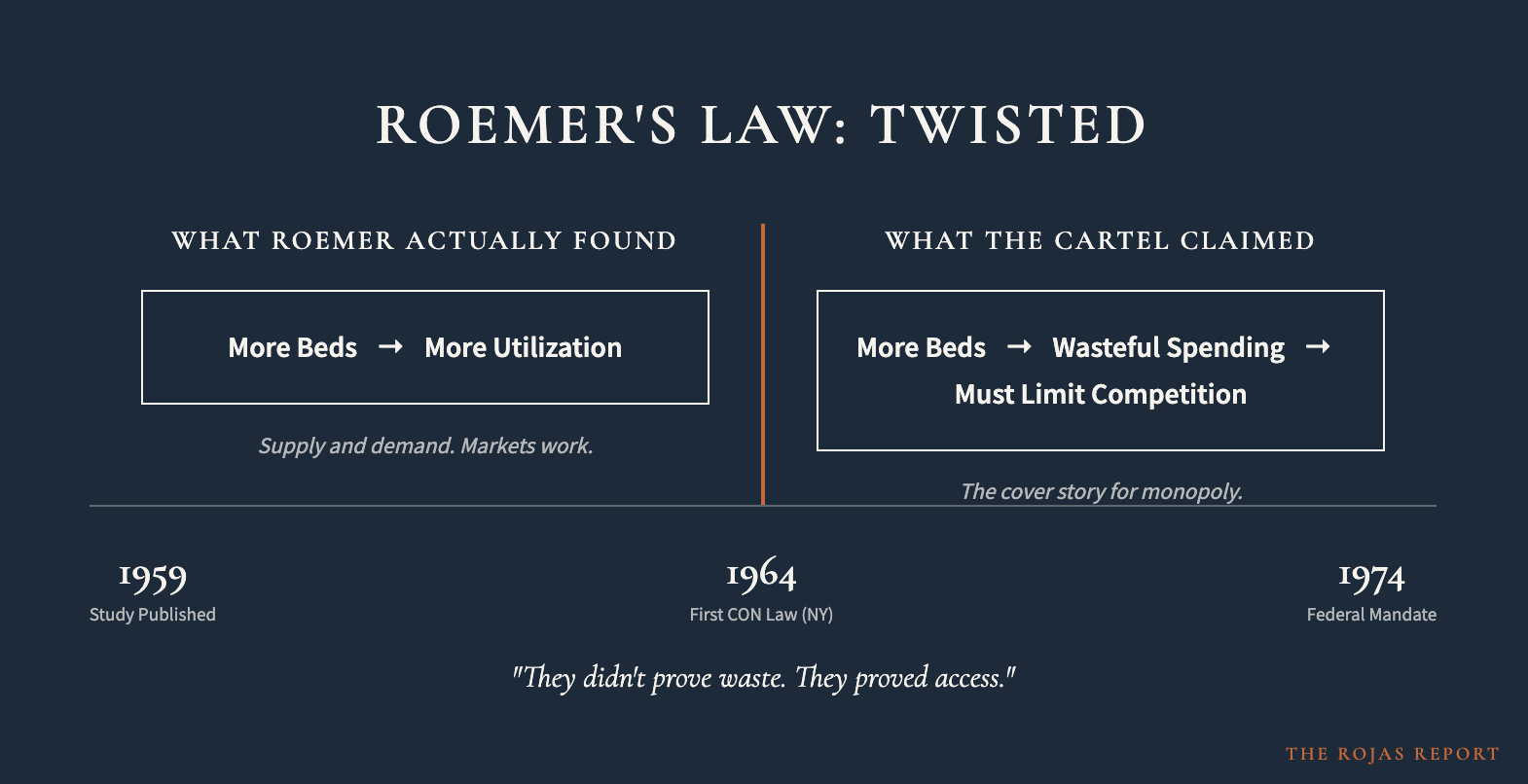
The story of CON laws begins in 1959 with a UCLA health researcher named Milton Roemer. His study found a correlation between the number of available hospital beds and the number of hospital days used. The hospital industry twisted this finding into a justification for limiting competition: if more beds mean more utilization, then we must restrict the supply of beds.
What Roemer actually proved was that supply and demand work. What the cartel claimed was that markets are wasteful and competition must be limited.
The federal government's entry into CON was the National Health Planning and Resources Development Act of 1974 (Public Law 93-641), sponsored by Senator Edward M. Kennedy. The law effectively federalized the CON concept, threatening to withhold federal funds from states that did not adopt CON programs. By the early 1980s, nearly every state had one.
The mandate was repealed in 1987 after the policy was deemed ineffective. But 35 jurisdictions kept their laws on the books.
They didn't prove waste. They proved access.
— The Rojas Report, on Roemer's Law
Roemer's study published at UCLA
New York enacts first CON law
AHA campaigns for nationwide CON
Federal mandate signed by Ford
Federal mandate repealed
35 jurisdictions still enforce CON
What CON Laws Actually Do
The Federal Trade Commission and the Department of Justice have found no reliable evidence that CON programs achieve any public benefits. They have found clear evidence that the laws grant anticompetitive benefits to protected business interests.
ASCs per 1 Million People
Same procedures. Fraction of the cost. Regulated out of existence.
Every State, Ranked
The Cicero Institute ranks all 50 states on the restrictiveness of their CON laws, scoring each from 0 (no CON) to 100 (most restrictive). Click any state with a full profile to see its investigation.
| Rank ↑ | State | CON Status | Score | Tier |
|---|---|---|---|---|
| 1 | Texas | No | 0 | Free Market |
| 1 | Idaho | No | 0 | Free Market |
| 1 | New Hampshire | No | 0 | Free Market |
| 1 | California | No | 0 | Free Market |
| 1 | Colorado | No | 0 | Free Market |
| 1 | Kansas | No | 0 | Free Market |
| 1 | New Mexico | No | 0 | Free Market |
| 1 | Pennsylvania | No | 0 | Free Market |
| 1 | South Dakota | No | 0 | Free Market |
| 1 | Utah | No | 0 | Free Market |
| 1 | Wyoming | No | 0 | Free Market |
| 1 | Arizona | No | 0 | Free Market |
| 14 | Florida→ | Repealed | 5 | Mostly Free |
| 14 | Montana→ | Limited | 5 | Mostly Free |
| 14 | North Dakota→ | Limited | 5 | Mostly Free |
| 14 | Ohio | Repealed | 5 | Mostly Free |
| 14 | Wisconsin→ | Limited | 5 | Mostly Free |
| 18 | Arkansas→ | Limited | 15 | Mostly Free |
| 18 | Indiana | Limited | 15 | Mostly Free |
| 20 | Oklahoma→ | Limited | 20 | Mostly Free |
| 21 | Minnesota→ | Yes | 30 | Moderate |
| 22 | South Carolina | Repealing | 35 | Moderate |
| 23 | Delaware→ | Yes | 45 | Moderate |
| 23 | Nebraska→ | Yes | 45 | Moderate |
| 25 | Alaska→ | Yes | 55 | Restrictive |
| 25 | Louisiana→ | Yes | 55 | Restrictive |
| 27 | Hawaii→ | Yes | 65 | Restrictive |
| 27 | Maine→ | Yes | 65 | Restrictive |
| 27 | Michigan→ | Yes | 65 | Restrictive |
| 27 | Illinois→ | Yes | 65 | Restrictive |
| 27 | Oregon→ | Yes | 65 | Restrictive |
| 27 | New York→ | Yes | 65 | Restrictive |
| 33 | Missouri→ | Yes | 80 | Highly Restrictive |
| 33 | Alabama→ | Yes | 80 | Highly Restrictive |
| 33 | Rhode Island→ | Yes | 80 | Highly Restrictive |
| 36 | Tennessee→ | Yes | 85 | Highly Restrictive |
| 37 | Mississippi→ | Yes | 90 | Highly Restrictive |
| 37 | Connecticut→ | Yes | 90 | Highly Restrictive |
| 37 | Iowa→ | Yes | 90 | Highly Restrictive |
| 37 | Massachusetts→ | Yes | 90 | Highly Restrictive |
| 41 | Georgia→ | Yes | 95 | Most Restrictive |
| 41 | Maryland→ | Yes | 95 | Most Restrictive |
| 43 | Kentucky→ | Yes | 100 | Most Restrictive |
| 43 | Nevada→ | Yes | 100 | Most Restrictive |
| 43 | New Jersey→ | Yes | 100 | Most Restrictive |
| 43 | North Carolina→ | Yes | 100 | Most Restrictive |
| 43 | Vermont→ | Yes | 100 | Most Restrictive |
| 43 | Virginia→ | Yes | 100 | Most Restrictive |
| 43 | Washington→ | Yes | 100 | Most Restrictive |
| 43 | West Virginia→ | Yes | 100 | Most Restrictive |
| 43 | District of Columbia→ | Yes | 90 | Highly Restrictive |
Source: Cicero Institute CON Restrictiveness Index. Scores range from 0 (no CON) to 100 (most restrictive).
The Architecture Stays
Everyone talks about PBMs. Everyone talks about insurer consolidation. Those are the visible villains. They get the press conferences and the bipartisan outrage. But the architecture that makes the monopoly possible is Certificate of Need. It is the foundation. It is the building the monopoly lives in.
The Break Up Big Medicine Act targets insurer-PBM-physician ownership, drug wholesaler-physician ownership, and vertical integration between payers and prescribers. It touches $0 of the $275 billion annual hospital subsidy apparatus. It ignores CON laws in 35 jurisdictions. It ignores the physician-owned hospital ban. It ignores $37.4 billion in nonprofit hospital tax exemptions. It ignores $81.4 billion in 340B program expansion.
The visible villains get a press conference. The architecture stays.
Deep-Dive State Profiles
These states have been fully investigated by The Rojas Report. Each profile includes market concentration data, case law, reform status, and the names of the systems that benefit from the monopoly.
Kentucky
Most RestrictiveThree systems control 100% of Louisville's inpatient market. Prices reach 354% of Medicare. A Nepali immigrant was blocked from serving refugees.
Virginia
Most RestrictiveSentara's $4.79B empire. Five systems control $16B+ in revenue. The 4th Circuit acknowledged the harm but refused to act.
Massachusetts
Highly Restrictive8 ASCs per million vs. 16+ national average. Mass General Brigham's $18.5B empire. A 15-year regulatory stranglehold on surgical competition.
Georgia
Most RestrictivePiedmont's $5.6B system. HB 1339 began reform in 2024. Centene controls 38% of the insurer market.
North Carolina
Most RestrictiveTwo systems control nearly 100% of Charlotte's inpatient market. BCBS NC holds 62% of the insurer market.
New York
RestrictiveNorthwell's $17.6B empire. 26 regulated services. The state that started it all in 1964.
Alabama
Highly RestrictiveDecatur HHI 10,000 — literal monopoly. BCBS Alabama controls 84% of the commercial market.
Mississippi
Highly RestrictiveA 40-year moratorium on new hospital construction. BCBS MS controls 53% of the insurer market.
New Jersey
Most RestrictiveRWJBarnabas Health's $7.5B empire. 25+ regulated services. The Garden State's healthcare cartel.
Illinois
RestrictiveBCBS controls 97% of the HMO market. CON law sunsets in 2029 — if the incumbents let it.
Florida
Mostly FreeMostly repealed, but hospice and nursing home CON remain. A court upheld a hospice monopoly in Sarasota.
Data sourced from Cicero Institute, National Academy for State Health Policy (NASHP), Federal Trade Commission, Department of Justice, Institute for Justice, Centers for Medicare & Medicaid Services (CMS), and individual state health departments.